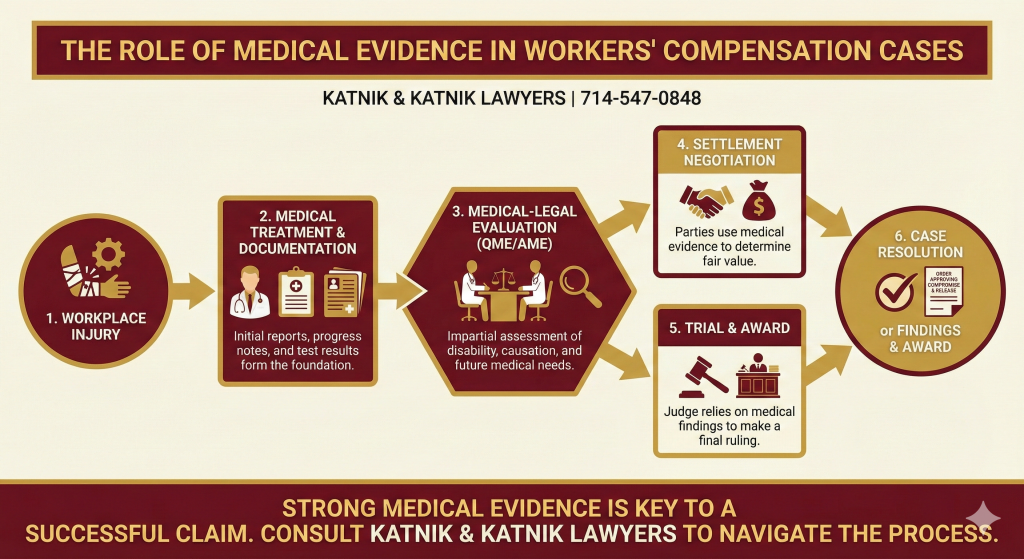
In football, every team relies on a detailed scouting report to understand their opponent’s strengths and weaknesses. This report dictates the game plan. In a workers’ compensation claim, your medical record is that scouting report. It tells the insurance company, the lawyers, and the judge everything they need to know about your injury. It determines whether you are cleared to get back on the field, need modified duties, or are permanently sidelined from the game. Understanding The Role of Medical Evidence in Workers’ Compensation Cases is the most critical factor in securing your benefits.
A weak or incomplete medical record is like a scouting report with missing pages. The defense—the insurance company—will exploit those gaps to deny treatment, minimize your disability rating, and force a lowball settlement. A strong, detailed, and legally sound medical record is your playbook for victory. It proves your injury, justifies the treatment you need, and secures the compensation you are owed. With over 65 years of experience in Santa Ana, we’ve seen thousands of cases hinge on the quality of these documents. This guide will break down how we build a championship-caliber medical record and protect you from the defense’s attempts to undermine your claim.
The Role of Medical Evidence in Workers’ Compensation Cases in California
Looking for more insight on building a compelling case? Read our related article on How to Strengthen Your Workers’ Comp Claim with Medical Evidence for practical strategies and tips.
In the California workers’ compensation system, not all medical opinions are created equal. To win your case, your doctor’s reports must meet the legal standard of substantial medical evidence workers’ comp California. This is a specific legal term that means the evidence is not just any opinion; it is an opinion that is well-reasoned, based on a thorough examination, and considers the full scope of your medical history and job duties.
What Makes Medical Evidence “Substantial”?
Think of it this way: a casual comment from a doctor is like a fan shouting from the stands. A substantial medical report is like the official review from the replay booth—it’s detailed, based on clear evidence, and determines the outcome of the play.
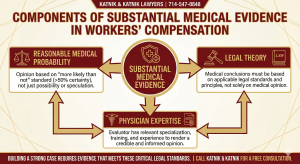
Essential Elements of a Substantial Medical Report
To be considered “substantial,” a medical report must include:
- Reasonable Medical Probability: Statements must be framed in legal-medical terms.
- Correct Legal Theory: The doctor must apply California labor laws correctly.
- Physician Expertise: Findings must be based on a physical examination performed by the doctor.
- Credible Complaints: The report must address the worker’s credible physical symptoms and history.
- Reasoned Analysis: The doctor must provide a clear, logical explanation linking the facts to the conclusions.
 A comprehensive report not only includes the doctor’s objective findings, like MRI or X-ray results, but also your reported symptoms, prior treatment, physical job description, and the physician’s medical judgment.
A comprehensive report not only includes the doctor’s objective findings, like MRI or X-ray results, but also your reported symptoms, prior treatment, physical job description, and the physician’s medical judgment.
Practical Application of Substantial Evidence
Example: Proper Documentation in Action
Suppose your treating physician documents decreased range of motion, persistent lower back pain radiating into the leg, and a positive MRI for a herniated disc. The doctor explains, with medical reasoning and citation to well-accepted guidelines, why these findings are work-related and require surgery. This form of documentation meets the substantial evidence standard and can be the difference between an approved surgery and a denial.
How Insurers Challenge Medical Evidence
If a report fails to meet this standard, a judge can throw it out. Insurance companies know this and will hire their own doctors to produce reports that look official but are designed to be flimsy. They will argue that your doctor’s report is not “substantial” and therefore should be ignored.
Common Tactics Used by Insurance Carriers
Insurance carriers may seize on gaps such as missing physical examination findings, ambiguous references to the cause of injury, or failure to explain how daily work led to your condition. In litigation, they often present reports by QME or AME physicians that introduce alternative explanations (“degenerative changes,” “age-related wear and tear”) with the specific intent of watering down your claim.
Legal Strategy: Strengthening the Medical Record
Skilled attorneys proactively counter these efforts by ensuring each treating physician’s report is as airtight as possible—if facts are lacking or ambiguous, we request a supplemental report, or even arrange a deposition to clarify the basis for the doctor’s opinion.
Case Study: Substantial Evidence Saves a Denied Claim
Consider Maria, a machine operator in Orange County, who injured her shoulder lifting boxes. The initial claim was denied on the grounds that her pain was consistent with “age-related degeneration.” Working together, we coordinated with her treating physician to prepare a detailed supplemental report that outlined the progression of her pain, work duties requiring repetitive overhead lifting, and objective findings on MRI. The physician cited the 2026 MTUS and ACOEM guidelines for shoulder injuries. This “substantial medical evidence” not only persuaded the QME, but also led to the judge awarding Maria wage loss and full medical treatment.
Safeguarding Your Claim with Comprehensive Reports
Our job is to ensure every medical report supporting your claim is bulletproof, meeting every legal requirement and leaving no room for the defense to attack. We audit every report to ensure it has the weight to stand up in court at the Santa Ana WCAB and win your case.
Qualified Medical Evaluator (QME) Process 2026
When you and the insurance company disagree on key medical issues—like the cause of your injury, the need for future treatment, or your level of permanent disability—the system calls in a neutral third party. This is the qualified medical evaluator (QME) process 2026. A QME is a physician certified by the state to perform these neutral evaluations. While they are supposed to be impartial, the QME process is a high-stakes play that can define the entire game.
The role of medical evidence in workers’ compensation cases is never more critical than during this evaluation. The QME’s report becomes the definitive “scouting report” that a judge will rely on to make final decisions.
What Does the QME Look For?
QMEs are mandated to review all available records, including PTP reports, diagnostic imaging, prior medical history, and even surveillance videos if provided. Their written opinions must explicitly answer questions about:
- The nature and extent of industrial injury
- Causation
- Permanent impairment ratings using AMA Guides
- Need for future care
- Work restrictions
Preparation Is Key: Building the Complete Medical Playbook
One misstep—failing to send a crucial operative report, for example—could lead to a QME finding against you. That’s why we methodically gather, index, and deliver every shred of relevant evidence to the provider well ahead of your appointment. We also send a cover letter framing the medical and legal issues, so the QME is primed to consider your case from our strongest angle.
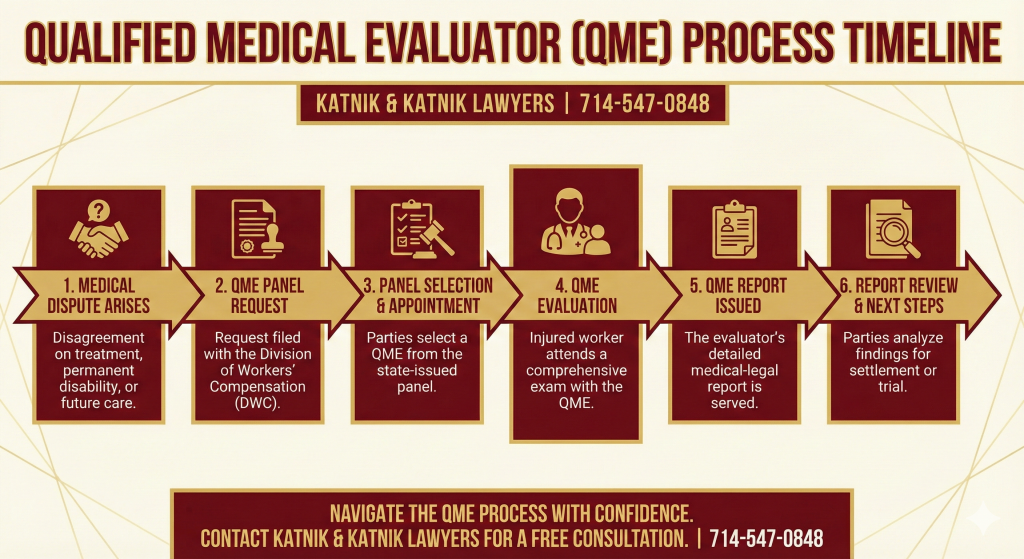
Timeline of the QME Process
Step | Action |
|---|---|
Dispute Arises | Disagreement between parties regarding a medical issue |
Panel Request | Application to DWC for three potential QME doctors |
Panel Selection | Parties strike doctors from panel until one remains |
QME Evaluation | Appointment takes place, all medical records reviewed, patient evaluated |
Reporting Deadline | QME must issue report within 30 days of evaluation |
Report Review | Parties receive QME report with detailed findings and opinions |
Objection Window | Opportunity to rebut or seek clarification within a set timeframe |
Example: QME as a Game Changer
After a denial for back surgery, one of our clients, an electrician, faced the insurance carrier’s “independent” medical opinion that conservative care was sufficient. We challenged this by organizing an extensive file for the QME, which included three years of physical therapy notes, pain journals, and MRI records. Our preparation led to a QME report that supported surgery based on a compelling record and the latest 2026 ACOEM guidelines. The claim was approved, demonstrating how proper QME handling—backed by robust medical evidence—wins difficult cases.
Medical Treatment Utilization Schedule (MTUS) Updates
In California, medical treatment is not authorized just because your doctor recommends it. Every treatment request must comply with the Medical Treatment Utilization Schedule (MTUS). The MTUS is the official rulebook for medical treatment in the California workers’ comp system. It is a massive set of guidelines, based on evidence-based medicine, that dictates what treatments are considered medically necessary for specific injuries.
An insurance company’s Utilization Review (UR) department will use the MTUS to approve or deny any treatment requested by your doctor. Understanding the latest MTUS updates is critical, as they change frequently and can directly impact your care.
Critical February 2026 MTUS Update
The Division of Workers’ Compensation (DWC) held a public hearing on February 27, 2026, to adopt critical updates to the MTUS. These changes directly affect two major areas of work injuries:
- ACOEM Chronic Pain Guideline: New, stricter standards for managing and treating chronic pain.
- ACOEM Eye Disorders Guideline: Updated protocols for treating occupational injuries to the eyes.
This update creates a new tripwire for injured workers. If a PTP’s request for treatment fails to cite these 2026 standards, UR will issue a denial. The insurance company will use this as a purely technical basis to deny necessary care, claiming the request was not compliant. We proactively educate our clients’ treating physicians on these updates, ensuring their requests are formatted correctly and reference the new guidelines, so you get the care you need without delay. We don’t let the insurance company win on a technicality.
Case Study: MTUS Misstep and UR Denial
A warehouse worker’s doctor requested a spinal cord stimulator for chronic pain after failed back surgery. The UR denied the request because the treatment justification did not cite the updated 2026 ACOEM guidelines. In response, we coordinated a supplement with the PTP, explicitly referencing the new standards and literature. Upon resubmission, the treatment was approved—demonstrating the impact of the 2026 MTUS changes and our due diligence as your legal team.
Key 2026 MTUS Guideline Updates
Update Area | Key Guideline Changes (Feb 2026) | Impact on Workers’ Comp Cases |
|---|---|---|
Chronic Pain | Adoption of updated ACOEM best practices for chronic pain management. | Stricter review of opioid prescriptions, surgeries, and device use. |
Eye Disorders | New ACOEM diagnostic and treatment pathways for job-related eye injuries. | Increased documentation and precise compliance now required. |
Submission Requirements | PTPs must cite 2026 ACOEM guidelines in all treatment requests. | Non-compliant requests face near-automatic utilization denials. |
Your Primary Treating Physician (PTP) is the quarterback of your medical team. This is the doctor you select to manage your day-to-day care. The reports they write are the foundation of your medical evidence. However, for these reports to be effective, they must comply with strict primary treating physician (PTP) reporting requirements.
Understanding PTP Reports: The Building Blocks
The PTP is responsible for issuing a series of reports at specific intervals:
- Doctor’s First Report of Occupational Injury or Illness (Form 5021): This is the opening play, submitted within 5 days of your initial visit. It establishes the injury and your initial diagnosis.
- Primary Treating Physician’s Progress Report (PR-2): This report is required every 45 days while you are actively treating. It updates your condition, work status, and treatment plan. A missed or late PR-2 gives the insurance company an opening to question your disability status.
- Primary Treating Physician’s Permanent and Stationary Report (PR-4): This is the final report issued when your doctor determines you have reached Maximum Medical Improvement (MMI). It must describe any permanent impairment using the AMA Guides, 5th Edition.
What happens if PTP requirements aren’t met?
If the reports are late, incomplete, or lack a detailed, reasoned analysis, the insurance company will pounce. They will stop your checks and deny your care. We work closely with our clients and their doctors to ensure these reporting requirements are met, creating a consistent, undeniable record of your injury and disability.
Successful Case: PTP Diligence Prevails
One client, a delivery driver, experienced several gaps between PR-2 reports due to switching doctors. When the insurance carrier stopped benefits, we immediately coordinated with the current PTP, who supplemented the record with detailed progress reports. Our efforts restored payments with retroactive benefits. Never underestimate the power and necessity of prompt, detailed PTP reporting.
Challenging a Denied Workers’ Comp Claim with Medical Records
When an insurance company denies your claim, they are essentially saying your medical evidence isn’t strong enough. The only way to fight back is by challenging a denied workers’ comp claim with medical records. This is a head-to-head battle where your medical file goes up against theirs.
Understanding Claim Denial Reasons
The initial denial letter will often state a reason, such as “the injury did not arise out of employment” or “there is no medical evidence of disability.” Overcoming these statements requires a deliberate and multi-front strategy.
Analyzing the Basis for Denial
1. Audit the Denial
We first analyze the basis for the denial. Did they rely on a biased report from one of their own doctors? Did they ignore key evidence from your PTP?
2. Gather Supplemental Evidence
We work with your PTP to obtain a supplemental report that directly refutes the insurance company’s reasoning. For example, if they claim your back injury is from a pre-existing condition, we get a report from your doctor explaining how your work duties “lit up” or aggravated that underlying condition, making it a compensable injury.
3. Utilize the QME Process
If the dispute remains, we initiate the QME process. This allows a neutral doctor to review all the evidence and issue a new, more powerful report that can override the insurance company’s initial denial.
4. Depositions and Cross-Examination
We can depose the insurance company’s doctor, forcing them to answer questions under oath about the flaws and biases in their report. We expose the weaknesses in their medical evidence for a judge to see.
Strategic Examples: Medical Evidence Overcomes Denial
Brian, a construction worker, developed knee pain after years on the job. His claim was denied due to “pre-existing arthritis.” We responded by collecting workplace incident logs, surveillance showing repetitive kneeling, and two clarifying PTP reports. A QME confirmed work causation based on this thorough medical and factual file, overturning the denial. The role of medical evidence in workers’ compensation cases was decisive.
The Strategic Role of a Strong Medical File
Your medical record is your ammunition in this fight. The more detailed, consistent, and well-reasoned it is, the better your chances of overturning that denial and securing your benefits.
When a Utilization Review (UR) doctor denies a specific treatment request from your PTP, your recourse is a process called Independent Medical Review (IMR). It is crucial to understand the difference between IMR vs QME, as they are used to solve different problems.
- QME (Qualified Medical Evaluator): Resolves disputes over legal and medical issues like causation of injury, permanent disability, and apportionment. The QME process decides the value of your case.
- IMR (Independent Medical Review): Resolves disputes only over the medical necessity of a specific treatment request denied by UR. IMR decides whether you get the surgery, physical therapy, or medication your doctor requested.
Table: IMR vs QME – Purpose and Process
Review Process | Issues Reviewed | Who Decides? | Outcome |
|---|---|---|---|
QME | Causation, permanent disability, apportionment | Neutral, state-certified physician | Legal impact on settlement, PD advances, benefits |
IMR | Medical necessity (treatment requests only) | Outside physician via DWC program | Determines authorization of treatment |
The Rodriguez v. WCAB Ruling (2026) and its Impact
For years, there was a legal gray area about whether you could use the QME process to get treatment authorized after a UR denial. That ended in 2026 with a landmark decision. The California Supreme Court’s 2026 review of Illinois Midwest Insurance Agency v. WCAB (Rodriguez) solidified the state’s position.
The new rule is clear: IMR is the exclusive path for medical necessity disputes, including ongoing care that was previously authorized, superseding the old Patterson doctrine. This means if UR denies your care, your only option is to appeal to IMR. You can no longer go to a QME to get that treatment authorized.
This ruling makes it even more critical that your PTP’s initial treatment request is perfect. Since you only get one shot with IMR, the request must be perfectly aligned with MTUS guidelines. The role of medical evidence in workers’ compensation cases now requires a proactive, strategic approach to treatment requests, because the old safety nets are gone.
Labor Code § 4628
Finally, for any med-legal report to be admissible as evidence—whether from a PTP, a QME, or another evaluator—it must comply with Labor Code § 4628. This law is designed to prevent fraud and ensure the doctor who signs the report is the one who did the work. The key requirements are:
- The physician must personally perform the non-clerical parts of the evaluation.
- The physician must sign the report under penalty of perjury.
- The report must disclose the location where the evaluation was performed.
We audit every med-legal report from both sides to ensure compliance. If an insurance company doctor’s report violates § 4628, we file a motion to have it thrown out, neutralizing the defense’s key evidence.
Example: Section 4628 at Work
An insurer’s QME submitted a report drafted largely by their non-physician assistant, with minimal direct evaluation. By highlighting the lack of compliance with § 4628 and demanding removal of the report from evidence, we sharply limited the defense’s ability to challenge our client’s benefits.
Frequently Asked Questions
Can the insurance company ignore my doctor’s MRI results?
A: No, they cannot ignore it, but they can dispute it. The insurance company will often have their own doctor (a radiologist) review the MRI scan and issue a competing opinion that downplays the findings. If your doctor sees a significant injury and their doctor sees “normal degenerative changes,” this creates a medical dispute that will likely need to be resolved by a QME. For more on how medical imaging is weighed in California workers’ comp cases, see our internal guide [Understanding Medical Imaging in Workers’ Comp](/unde
What if the QME report is full of mistakes?
A: This is a common and serious problem. If a QME report contains factual errors (like listing the wrong date of injury or misquoting your job duties), we can request a supplemental report from the QME to correct the errors. If the QME’s medical reasoning is flawed, we can depose the doctor to challenge their conclusions under oath. Exposing these mistakes is key to undermining a bad report. For a step-by-step process, see What to Do When the QME Gets It Wrong and review California DWC QME guidelines.
Why was my surgery denied if my doctor said I need it?
A: Your surgery was likely denied by Utilization Review (UR) because the request from your doctor was deemed not medically necessary under the MTUS guidelines. This could be due to a technical error in the request or a disagreement over the clinical findings. Your only recourse after a UR denial is to file for an Independent Medical Review (IMR) within 30 days. Read our IMR survival guide or consult the California Department of Industrial Relations IMR page for official procedures.
Q: Can the insurance company ignore my doctor’s MRI results?
A: No, they cannot ignore it, but they can dispute it. The insurance company will often have their own doctor (a radiologist) review the MRI scan and issue a competing opinion that downplays the findings. If your doctor sees a significant injury and their doctor sees “normal degenerative changes,” this creates a medical dispute that will likely need to be resolved by a QME. For more on how medical imaging is weighed in California workers’ comp cases, see our internal guide Understanding Medical Imaging in Workers’ Comp or our article Common Workplace Injuries and California Claim Strategies. For further reading, review guidance from the Radiological Society of North America (RSNA) and California DWC Medical Unit.
Q: What if the QME report is full of mistakes?
A: This is a common and serious problem. If a QME report contains factual errors (such as listing the wrong date of injury or misquoting your job duties), we can request a supplemental report from the QME to correct those mistakes. If the QME’s medical reasoning is flawed, we can also depose the doctor to challenge opinions under oath. For a detailed process, review our article What to Do When the QME Gets It Wrong and examine official California DWC QME guidelines. For more on doctor disputes, see our guide How to Challenge an Unfavorable QME Report.
Q: Why was my surgery denied if my doctor said I need it?
A: Your surgery was most likely denied by Utilization Review (UR) because the request from your physician was deemed not medically necessary under MTUS guidelines. This could arise from a technical error or a disagreement over clinical evidence. After a UR denial, your only recourse is to file for an Independent Medical Review (IMR) within 30 days. Read our IMR Survival Guide, our in-depth article How to Appeal a Denied Workers’ Comp Treatment Request, or consult the California Department of Industrial Relations IMR page for official procedures and requirements.
The role of medical evidence in workers’ compensation cases is absolute. Your future—your ability to get medical care, your disability payments, and your final settlement—all comes down to the quality of the reports in your file. Insurance companies have entire teams dedicated to finding flaws in your medical record to save money. You need a team that is just as dedicated to building an ironclad case for you.
At Katnik & Katnik Lawyers, we don’t just read medical reports—we audit them for legal compliance, medical accuracy, and strategic strength. We collaborate with your doctors to ensure every detail is correct, building a record the defense cannot undermine. Put our 65-year legacy to work for your case.
Ready to protect your claim?
